Background
The lumbar spine consists of five vertebrae in the lower back, and it is crucial for supporting much of the upper body’s weight and it helps facilitate various movements in the body. Intervertebral disks work as separators so that when a person moves, the bones of their vertebrae don’t rub against each other and break [13]. Disk degeneration occurs, causing the disk to wear out and become non-functional (Figure 1A).
The current standard care option is to perform spinal fusion which removes the degenerated disk and welds the vertebrae together, in order to diminish pain associated with the rubbing of the bones. Recently, there has been a spike in research for an artificial disk that could replace the damaged one, thereby removing the need for spinal fusion surgery [2]. Despite the existing research, no artificial disks have produced significant clinical outcomes. Furthermore, there has not been any specific testing done on the L5-S1 disk due to the complicated nature curvature that exists in the body and the amount of shear force that it sustains. A disk that was created for the cervical spine could not be easily repurposed for the lumbar spine due to the angle and asymmetrical nature of the L5-S1 disk. Within the L5-S1 region, this intervention is most needed as there is the greatest sign of reduced signal intensity and degeneration but it also has the highest percentage of grade 3 disk degeneration (Figure 1B) [14].

Figure 1: (A) L5-S1 region of spine in the body (left) and diagram showing herniation of the L5-S1 disk (right) [15]. (B) Signal intensity of lumbar discs (diseased and normal) at various lumbar levels [14].
Degenerative disk disease can cause problems such as scoliosis, herniated disk, spinal stenosis or spondylolisthesis. It is most commonly found in adults over the age of 40 and some factors that increase the development of disk degeneration are acute injuries, obesity, smoking and physically demanding exercise [21].
Market
The artificial disk replacement market has grown over the last few years and is projected to continue increasing for the next five (Figure 2). Investments also increase for spinal injuries due to the prevalence in the athlete population because athletes are willing to pay more money than the average person for medical treatment and innovation. Furthermore, almost half of athletes with disk replacements regain the ability to return to their sport unrestricted [22]. This is advantageous since previously, degenerative disk disease would require spinal fusion, which is a career ending surgery.

Figure 2: Projected growth of North American artificial disk replacement market from 2018 to 2028 [1].
Additionally, the market is rapidly expanding due to the increasing aging population. On average, people are now living longer worldwide. Since disk degeneration can also occur through natural wear and tear over time, the need for disk replacements will continue to grow with the growth of the older population. Since there are no current L5/S1 disk replacements on the market with significant results, there has been hesitation to use them in older patients due to the long recovery time and decreased activity. However, a long-lasting device without need for readjustments would benefit this age group and improve one’s quality of life.
Key Stakeholders
Patients are the key stakeholders of our device. Low-back pain (LBP) is one of the most common health problems reported in primary care [22]. Not accounting for indirect costs associated with the loss of productivity and unemployment, the estimated cost of managing LBP in the US per year is between $12 billion and $91 billion with the economic implication of healthcare costs to Americans amounting to approximately 50 billion annually. [10] The most common causes of lower back pain are related to complications and disorders of the L5-S1 segment of the back with a close second being the L4-L5 region. [15]
Healthcare providers are essential in being the touchpoint between the device manufacturers and the patients themselves. Within the United States, “back pain is the fifth leading cause of admission to the hospital and the third most common indication for surgical procedures. [12] From a non-surgical perspective, providers are crucial in determining whether a patient should undergo artificial disk replacement or opt for alternative treatment. However, once a patient is deemed suitable and favorable for artificial disk replacement, particularly in the L5-S1 region, the selection of the appropriate type of artificial disk and planning the surgical intervention is created.
With regards to medical device manufacturers, noble entities within this sector are Medtronic, Orthofix Medical Inc., Globus Medical, and NuVasive, Inc., Johnson & Johnson among others. These entities are engaged in a variety of strategic initiatives such as product development, pre and post clinical trials, expansion of distribution network etc. thereby aiming to enhance market growth and development. These companies are contributing to the speculated compound annual growth rate of 18.4% between 2022 and 2029 reaching nearly $8.66 billion by 2029. It is easy to presume that the relatively high success rate of artificial disk replacements are leading the rapid industry expansion.
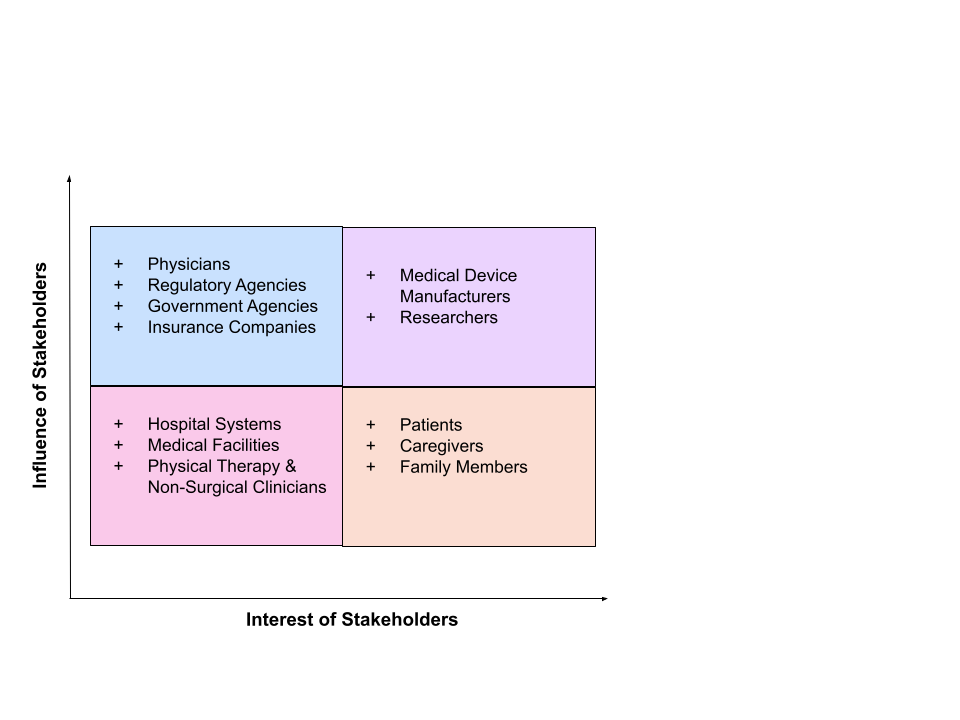
Figure 3: Stakeholder map for lumbar artificial disk device.
Client Justification
Our client is appropriate for this project because they are medical school students who are passionate about helping people and have done extensive research on disk replacements in the cervical spine. Our client has the resources and dedication to help us achieve our goals and complete this project. Furthermore, our client recognizes both the pressing need and untapped market share within this product.
Need Statement
There is a need to develop a long-term, minimally invasive treatment for patients
experiencing a degenerative disk disease or injury, such as spondylolysis or a herniated
disc, in order to relieve pain in the lumbar spine and restore movement and stability.
Project Scope
A pressing need exists for the development of a sustainable, minimally invasive treatment option for patients with degenerative disk disease or injuries such as spondylosis or a herniated disc, in order to relieve pain in the lumbar and sacral regions of the spine and thereby restore movement and stability. The designers/developers propose the following specifications for the prototype of an artificial disk, slated for delivery on the final day of class in April of 2024. Such specifications of the prototype include but are not limited to:
- Allows for the replacement of the L5-S1 spinal joint, thereby enabling adjacent spinal vertebrae to press together.
- Proper integration is ensured to prevent dislocation of the artificial disk to unintended areas of the body.
- Proper integration to maintain possible inward curves towards the spine. [14]
- Sustains shear and translational forces further than compression.
- Allows for natural range of motion including flexion and extension in the sagittal plane, lateral bending in the frontal plane, and rotation and compression in the axial plane. [11]
- Restricts translation and sliding of the disk beyond the normal range of motion and prevents vibration; thereby able to bear the load of the body.
- Is composed of a material that is biocompatible and possesses elastic resistance to optimally absorb a wide variety of shocks reverberating throughout the spine.
A 3D printed model will be developed thereby serving as a physical prototype. Subsequently, the project plans to adhere to comprehensive evaluations of the prototype, utilizing both finite element analysis and modeling to ensure the integrity and functionality of the product. Important to note, forms of the prototype along with its subsequent iterations, will undergo rigorous physical examinations to assess its resilience against pertinent compressive, shear and translational forces. These assessments thereby aim to validate the capacity of the prototype in congruence to physiological specification, as well as refine the design for optimal performance.
Design Specifications
- Sustain shear forces up to 700 N in the anterior-posterior direction. [8]
- Sustain compression forces up to 2000 N in the upright (0 degrees) position. [16]
- Sustain compression forces up to 3400 N for small trunk flexion angles (30 and 45 degrees).
- Provide six degrees of freedom and tri-planar motion.
- Thickness/height of 6.15-10.33 ± 1.0 mm with an angle of 15.28 degrees [5].
- Width of 55.37-58.60 ± 2.0 mm dependent on patient’s physiology.
- Anteroposterior diameter of 15.5 ± 1.5 mm depending on the age and gender status of the patient/client [11].
- Weight of approximately 20 ± 5 g [18,20].
- Cost of approximately $10,000 [3].
- Plate adherence mechanics requirements, such as minimal slippage and compression and shear forces.
- Biocompatibility in the L5-S1 spinal region.
Existing Solutions
Many patents exist for intervertebral disk implants and prosthetics. In 2006, SDGI Holdings Inc. submitted a patent for an intervertebral prosthetic disk that can be inserted between any two vertebrae (Figure 4A). The device consists of superior and inferior support plates, consisting of bearing surfaces and articular surfaces, and a hemispherical projection that extends from the superior articular surface of the support plate. The inferior articular surface has a hemispherical depression to receive the projection from the superior plate. Due to the projection, the superior layer of the device can be conformed to the shape of the superior vertebra, while the inferior layer engages the inferior vertebra. The compliant layers are molded to match the shape of the cortical rim and cancellous bone of the surrounding vertebrae. This increases the contact area between the vertebrae and plates, which reduces contact stress [9].
Only months later, DePuy Spine LLC submitted a patent for their intervertebral prosthetic disk with a shear-limiting core (Figure 4B). This design is very similar to that of SDGI Holdings Inc., although the hemispherical projection has been replaced with a central disk and radial flange. The central disk includes superior and inferior bearing surfaces, and the radial flange includes a radial extension from the central disk and an inferior axial extension from the outer edge of the flange. The axial extension of the flange connects to the inferior plate, restricting it from rotating in the flexion and lateral bending planes. The primary material used is ultra high molecular weight polyethylene, which has a high resistance to wear. The device is attached to the surrounding vertebrae via osteoconductive teeth [6].
DePuy Spine LLC has since evolved into DePuy Synthes Products Inc., which filed for application of an updated intervertebral implant with a conformable endplate in 2019 (Figure 4C). The superior and inferior endplates can conform to the vertebral endplate under anatomical load. There is a core between the endplates as opposed to the radial flange from the 2006 design, which provides relative movement of the endplates in accordance with the surrounding vertebrae. The core-endplates design is now the market standard for both cervical and lumbar disk implants [17].
Many of the most recent patents for intervertebral artificial discs follow similar designs and structures to those above, as well as designs on the market. The CHARITÉ Artificial Disc was the first total disk replacement approved for the market (Figure 4D) [7], which has recently been replaced by an updated design, the INMOTION. Both consist of two highly polished metal endplates with an ultra high molecular weight polyethylene (UHMWPE) core. The endplates have pointy extrusions on the edges to adhere to the surrounding vertebrae, and the endplates are porous so that bone can grow into the device [23]. This was one of the few devices primarily used for the lumbar spine, although it is no longer still on the market.
The Prodisc-L Total Lumbar Disc Replacement also utilizes the plates-and-core design, with cobalt chrome alloy endplates and a UHMWPE core (Figure 4E) [4]. Both endplates were plasma-sprayed with titanium for bone integration, in addition to the pointy extrusions along the midline. Tens of thousands of patients have received this disk at one level since its release in 2005, and the FDA recently approved the device for two-level vertebral disk disease [23].
The activL Artificial Disc is the third most common lumbar disk implant (Figure 4F) [24]. The cobalt-chromium endplates and UHMWPE core make this device similar to the Prodisc-L, UHMWPE being the most common core material for artificial discs throughout the spine. The activL differs by its curved superior surface of the core, allowing for enhanced structural support and range of motion. This device has a lower thickness than comparable disk implants, and the manufacturers produce a variety of endplate sizes to fit patient anatomy. The activL is one of few implants primarily used in patients with degenerative disk disease at the L5/S1 disk [23]. It is important to note that the above devices all have significant complications, can involve invasive insertion procedures, and may need to be replaced frequently.

Figure 4: (A) Sketch of Intervertebral Prosthetic Disc from SDGI Holdings Inc. patent, 2006 [9]. (B) Sketch of Intervertebral Prosthetic Disc with Shear-limiting Core under asymmetrical compression from DePuy Spine LLC patent, 2006 [6]. (C) Intervertebral implant with Conformable Endplate under asymmetrical compression in DePuy Synthes Products Inc. patent, 2019 [17]. (D) Image of CHARITÉ Artificial Disc [23]. (E) Image of Prodisc-L Total Lumbar Disc Replacement [23]. (F) Image of activL Artificial Disc [23].
Team Responsibilities
Group responsibilities will be primarily distributed based on each team member’s skill set, if possible. Sophie has the most experience working with joints, due to her work with Dr. Farshid Guilak on osteoarthritis. As such, she focuses on the biomechanics of the intervertebral disk and the structure of existing artificial discs, and will develop a stress strain mechanism prototyping. Camila has experience with material science, due to her chemical engineering courses. Thus, she primarily researches various materials and the requirements of the device, and will test materials during the prototyping stage. Evie has a neurology background, meaning that she best understands the nerve structure of the spinal cord and more of the biology side. She also has worked with different companies through internships and connections with industry, so she will do most of the market and stakeholder analysis. The gantt chart below reflects division of work in accordance with each team member’s strengths, and which aspects of the project will be a fully joint effort (Figure 5).
Design Schedule

Figure 5: Gantt chart for Senior Design Project, showing primary team member assignments, start and end dates, and progress on each element.
References
[1]Artificial Disc Replacement Market Size Report, 2021-2028. (n.d.). https://www.grandviewresearch.com/industry-analysis/artificial-disc-replacement-market-report.
[2]Artificial disk replacement in the lumbar spine – orthoinfo – aaos. OrthoInfo. (n.d.). https://orthoinfo.aaos.org/en/treatment/artificial-disk-replacement-in-the-lumbar-spine/.
[3]Buttacavoli, F. A., Delamarter, R. B., & Kanim, L. E. (2010). Cost comparison of patients with 3-level artificial total lumbar disc replacements versus 360° fusion at 3 contiguous lumbar vertebral levels: an analysis of compassionate use at 1 site of the US investigational device exemption clinical trial. SAS journal, 4(4), 107–114. https://doi.org/10.1016/j.esas.2010.07.002.
[4]Centinel Spine: For Prodisc® Motion-Preservation/Disc Arthroplasty and STALIF® Integrated Interbody Fusion Spine Surgery Solutions.” Centinel Spine | For Prodisc® Motion-Preservation/Disc Arthroplasty and STALIF® Integrated Interbody Fusion Spine Surgery Solutions, www.centinelspine.com/prodisc_l.php. Accessed 28 Sept. 2023.
[5]Disc spaces, vertebral dimensions, and angle values at the lumbar region: a radioanatomical perspective in spines with L5–S1 transitions. Journal of Neurosurgery: Spine, 15(4), 2011.
[6]Dooris, A., Rogers, C., & Parsons, M. (n.d.). Intervertebral disc prosthesis with shear-limiting core. Patent Number: US7909876B2.
[7]Fred H. Geisler (2006). The CHARITÉ Artificial Disc: Design History, FDA IDE Study Results, and Surgical Technique. Clinical Neurosurgery 53(24). 223-228.
[8]Gallagher, S., & Marras, W. S. (2012). Tolerance of the lumbar spine to shear: a review and recommended exposure limits. Clinical biomechanics (Bristol, Avon), 27(10), 973–978. https://doi.org/10.1016/j.clinbiomech.2012.08.009.
[9]Heinz, E., & Trieu, H. (n.d.). Intervertebral prosthetic disc. Patent number: US20070179618A1.
[10]Hoy, D., Brooks, P., Blyth, F., & Buchbinder, R. (2010). The epidemiology of low back pain. Best Practice & Research Clinical Rheumatology, 24, 769–81.
[11]Lazennec, J. Y. (2020). Lumbar and cervical viscoelastic disc replacement: Concepts and current experience. World Journal of Orthopedics, 11(8), 345–356. https://doi.org/10.5312/wjo.v11.i8.345.
[12]Levin, D. A., Bendo, J. A., Quirno, M., Thomas, E., Godlstein, J., & Spivak, J. (2007). Comparative charge analysis of one- and two-level lumbar total disc arthroplasty versus circumferential lumbar fusion. Spine, 32, 2905–9.
[13]Lumbar Disk Replacement. Johns Hopkins Medicine. (2021, May 3). https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/lumbar-disk-replacement#:~:text=In%20general%2C%20lumbar%20disk%20replacement,You%20are%20not%20excessively%20overweight.
[14]Medical Advisory Secretariat. (2006). Artificial discs for lumbar and cervical degenerative disc disease – update: an evidence-based analysis. Ontario Health Technology Assessment Series, 6(10), 1–98. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1724651/pdf/v037p00263.pdf.
[15]MyChiro. (n.d.). L5 S1 Disc Bulge – Causes, Symptoms, Treatment & Prevention. https://www.mychiro.com.my/articles/l5-s1/ .
[16]Navid Arjmand, Mohammad Amini, Aboulfazl Shirazi-Adl, André Plamondon, Mohammad Parnianpour, Revised NIOSH Lifting Equation May generate spine loads exceeding recommended limits, International Journal of Industrial Ergonomics, Volume 47, 2015, Pages 1-8,ISSN 0169-8141, https://doi.org/10.1016/j.ergon.2014.09.010.
[17]O’Niel, M. (n.d.). Expandable intervertebral implant and related methods. Patent Number: US20200015982A1.
[18]Othman, Y. A., Verma, R., & Qureshi, S. A. (2019). Artificial disc replacement in spine surgery. Annals of translational medicine, 7(Suppl 5), S170. https://doi.org/10.21037/atm.2019.08.26.
[19]Panda , S., & Arora, G. (2015). Evaluation of canal stenosis of herniated lumbar disc and its correlation to anterior-posterior diameter with magnetic resonance imaging morphometry. https://www.ijhas.in/article.asp?issn=2278-344X;year=2015;volume=4;issue=4;spage=253;epage=258;aulast=Panda.
[20]Physical properties for UHMW sheet. Physical Properties for UHMW Sheet | U.S. Plastic Corp. (n.d.). https://www.usplastic.com/knowledgebase/article.aspx?contentkey=549.
[21]Professional, C. C. medical. (n.d.). Degenerative disk disease: Causes, symptoms & treatment. Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/16912-degenerative-disk-disease.
[22]Rapoport, J., Jacobs, P., Bell, N. R., & Klarenbach, S. (2004). Refining the measurement of the economic burden of chronic diseases in Canada. Chronic Diseases in Canada, 25(1), 13–21. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2219656/
[23]Types of artificial disc replacement. Spine Surgery. (n.d.). https://www.spine.md/artificial-disc-replacement/types-of-artificial-disc-replacement/.
[24]U.S. Food and Drug Administration. (n.d.). activL® Artificial DiscPatient Information. Retrieved from https://www.accessdata.fda.gov/cdrh_docs/pdf12/P120024d.pdf.