Exploring Endovascular Treatments for Wide-Neck Bifurcation Aneurysms
Group 13 | 27 September 2024
Aaron Peters, Jenna Nguyen, Riya Bhakta
Background
Advancements in endovascular technologies have significantly improved aneurysm treatment, offering surgeons less invasive alternatives compared to traditional open surgery. Procedures such as coiling and stenting have become more refined, providing solutions for many patients with simpler aneurysm cases. However, wide-neck middle cerebral artery (MCA) bifurcation aneurysms remain a substantial challenge. These aneurysms are particularly difficult to treat due to their high-flow dynamics and the involvement of critical blood vessels that branch off near or directly from the aneurysm itself. These structural and physiological complexities often make endovascular techniques less effective or even unviable in many cases. As a result, open surgery is still frequently required for these types of aneurysms, despite the advances in less invasive procedures. Open surgery, while effective, carries its own risks, including longer recovery times and higher chances of complications, especially given the aneurysm’s proximity to critical brain structures.
Intracranial aneurysms affect an estimated 2-4% of the population, with a significant number of these occurring in the MCA bifurcation, which accounts for 18-36% of all intracranial aneurysms.1 This condition is most commonly found in adults aged 30 to 60 and occurs more frequently in women than in men.2 Wide-neck MCA bifurcation aneurysms, in particular, pose a significant risk of severe neurological complications including stroke or hemorrhage if left untreated. Without treatment, these aneurysms can rupture, leading to significant brain damage or even death.
Many patients face the issue of undergoing more complex and invasive surgical procedures, which increases both healthcare costs and the risks associated with surgery. Given the complexity and the critical nature of these cases, it is most practical to focus on innovative treatment methods that can minimize the need for open surgery. In the United States alone, an estimated 6,000 to 7,500 bifurcation aneurysms are treated surgically each year, with an average cost of $45,493 per procedure.3 These procedures not only present a high financial burden to the healthcare system, but they also place a significant strain on patients and their families.
New treatment solutions that can overcome the limitations of current endovascular approaches could greatly reduce the need for open surgery and improve patient outcomes. Developing new, more effective treatments could not only improve survival and recovery rates but also reduce the overall financial impact on both patients and healthcare providers. This makes the development of novel, minimally invasive treatments a priority in both medical research and healthcare policy.
Need Statement
Neurosurgeons need a way to endovascularly reduce the risk of aneurysm rupture in MCA bifurcation aneurysms to improve patient outcomes and enhance the safety of surgical interventions.
Project Scope
Neurosurgeons need a way to endovascularly reduce the risk of aneurysm rupture in MCA bifurcation aneurysms to improve patient outcomes and enhance the safety of surgical interventions. Current endovascular methods are insufficient for treating MCA bifurcation aneurysms, often requiring open surgery. One proposed solution to reduce the risk of rupture is an endovascular spiral device that alters blood flow dynamics upstream of the aneurysm, offering a viable alternative for these complex cases. Developing this new treatment method would provide patients with more consistent outcomes. This device must be compressible to a diameter of at most 1 mm, a length of at most 3 mm, and a cost of at most $1,200. Preliminary simulations, a physical quantitative model, a to-scale prototype device, a design notebook, validation & verification results, and manufacturing methodology will be available to our client, Sam Brehm, by April 28th, 2025.
Client Justification
Sam Brehm is a third-year medical student at Washington University School of Medicine who is currently pursuing an MBA alongside his medical education. In addition to his academic goals, Sam conducts clinical neurosurgery research under the mentorship of Dr. Camilo Molina and Dr. Jacob Greenburg. The combination of clinical and business knowledge positions Sam to be a valuable collaborator in the development of a novel solution for treating complex aneurysms. Sam provides the necessary resources and expertise to guide the project toward success, and his deep understanding of the neurological field allows him to recognize clinical needs and evaluate the existing market.
Key Stakeholders
The development of a device for endovascular treatment of wide-neck MCA bifurcation aneurysm has multiple key stakeholders to consider. The key stakeholders with low interest and low power are the suppliers and manufacturers of the device and competitor device companies. Suppliers and manufacturers of the device have the sole purpose of producing the device and do not readily influence the device design. The key stakeholders with low interest but high power include investors, the Sling Health team, and insurance companies. Serving as a source of funding and resources, these stakeholders are influential, but they have low interest in the details of device development other than hoping for success.
The stakeholders with high interest but low power are physicians, wide-neck MCA bifurcation aneurysm patients, and their family members. Physicians are the primary users of the device and hope for better patient outcomes and a simpler workflow as a result of successful device development. As direct recipients of the device, patients stand to gain the largest benefit from development success. Families of wide-neck MCA bifurcation aneurysm patients gain peace of mind in the safety of their loved ones from the device. However, these stakeholders do not have the ability or bandwidth to develop this solution themselves, making them all high interest but low power. The stakeholder with both high interest and power is the client, Sam Brehm. The original idea for the device comes from the client who serves as a mentor to the project and has a high personal interest in the project’s success. The client also guides the selection of the final solution’s form factor and materials, making the client have both high interest and power.

Figure 1: Key stakeholder map
Design Specifications
An endovascular treatment method for wide-neck MCA bifurcation aneurysms must be compressible such that it can be threaded through the body without damage to vessels serving as a passage for the treatment. Thus, the diameter of the compressed device, uncompressed device, and device applicator were chosen such that the device can be safely inserted into the applicator and threaded into the brain.4 The uncompressed diameter should conform to the vessel in which it is inserted to stabilize the device. Since cerebral vessels can vary in different patients, a range is provided for the device diameters.5 If the final device is a flow diverter with a spiral geometry, the angle of twist and the device length should be 45 degrees and 3mm, respectively; this is based on preliminary simulations done to test the effectiveness of a spiral flow diverter on flow in the aneurysm environment. These simulations were also used to determine the metrics for flow and surface pressure reduction. More information about these simulations can be found in the appendix under preliminary simulations. The elastic modulus of the device material was chosen because the device must be very elastic such that its original shape is immediately recovered upon removal of a compressive force. Since wide-neck MCA bifurcation aneurysms affect mainly people aged 30-60,2 the device lifespan must be at least 50 years such that it survives throughout the patient’s lifetime. Tolerances were added to design specifications based on a range that the metric could reasonably take on without harm to the patient. The cost of the device and the applicator was determined based on6,7 the price of similar devices on the market such as stents and stent applicators.
Table 1: Design Specifications with Metrics
| Specification | Metric | |
| Geometry | ||
| Diameter | Outer Device (Compressed) | < 1 mm |
| Outer Device (Uncompressed) | 2 mm – 5 mm | |
| Inner Device Applicator | > 1 mm | |
| Angle of Twist | 45-degree +/- 0.1 degrees | |
| Length | 3mm +/- 0.01mm | |
| Material Properties | ||
| Young’s Modulus | <70 GPa | |
| Performance | ||
| Fluid Flow Reduction into Aneurysm Head | >40% | |
| Aneurysm Head Surface Pressure Reduction | >20% | |
| Device Lifespan | >50 years | |
| Overall Cost | ||
| Device Cost | <$1,100 | |
| Applicator Cost | <$200 | |
Existing Solutions
Generally, traditional endovascular treatment was most adequate for resolving MCA bifurcation aneurysms.3 However, future endovascular techniques can still be useful in treating MCA bifurcation aneurysms. Descriptions of alternative techniques and some of their associated drawbacks are summarized below in Table 2.
Table 2: Existing solutions accompanied by a description and limitations of these solutions.8,9
| Endovascular Treatment Type | Description |
| Single Coiling | Single coiling is the best choice for MCA aneurysm treatment. However, even with the assistance of a balloon or dual-microcatheter, the embolization may be incomplete. |
| Stent-Assisted Coiling | Improves on techniques utilized in single coiling, resulting in an improved success rate. Despite this, stent-assisted coiling increases the risk of procedure-related complications. |
| Parent Artery Occlusion | Not a common technique due to ischemic balancing complications. |
| Women Endobridge Device | Proven feasible for treatment of MCA bifurcation aneurysms, however not suitable for every MCA aneurysm. Additionally, it has only been tested in select cases. |
| pCONus Device | A self-expanding device that is placed within the aneurysm to facilitate more effective coil placement. Concerns exist regarding deployment and thromboembolic complications. |
| Flow Diversion | For saccular aneurysms, flow diverter deployment offers a high rate of occlusion. However, the procedure-related ischemic complications must be considered due to the high rate of perforating arteries by the flow diverter. |
Preliminary Design Schedule
A GANTT chart was created representing the preliminary design schedule including tasks for the semester, task owners, task start and end dates, percent completion of each task, and the date of last update. The GANTT chart also includes a task distribution manager that auto-populates with updated task counts per person as new tasks are assigned to a task owner. The GANTT chart for the Fall 2024 and Spring 2025 semesters is shown below in the appendix.
Team Responsibilities
Individual responsibilities were assigned, and can be seen in Table 3, based on team members’ interests and equal distribution. While all team members contributed to the major reports and presentations, certain individuals were assigned responsibilities to oversee deadlines and ensure that contributions were made by each member. Attendance at weekly meetings is expected of all members to maintain accountability and continuous progression of the project.
Table 3: Brief information on what each member of the team will take the lead on.
| Team Member | Individual Responsibilities |
| Aaron Peters | Prototype (Physical Simulation)Data CollectionVerification and Validation PresentationSling Health LeadPreliminary, Progress and Verification and Validation ReportsFinal Report |
| Jenna Nguyen | Progress PresentationVirtual SimulationsPreliminary, Progress and Verification and Validation ReportsFinal ReportWebpage Manager |
| Riya Bhakta | Preliminary Presentation Scaled PrototypeDesign Notebook ManagerPreliminary, Progress and Verification and Validation ReportsFinal Report |
Appendix
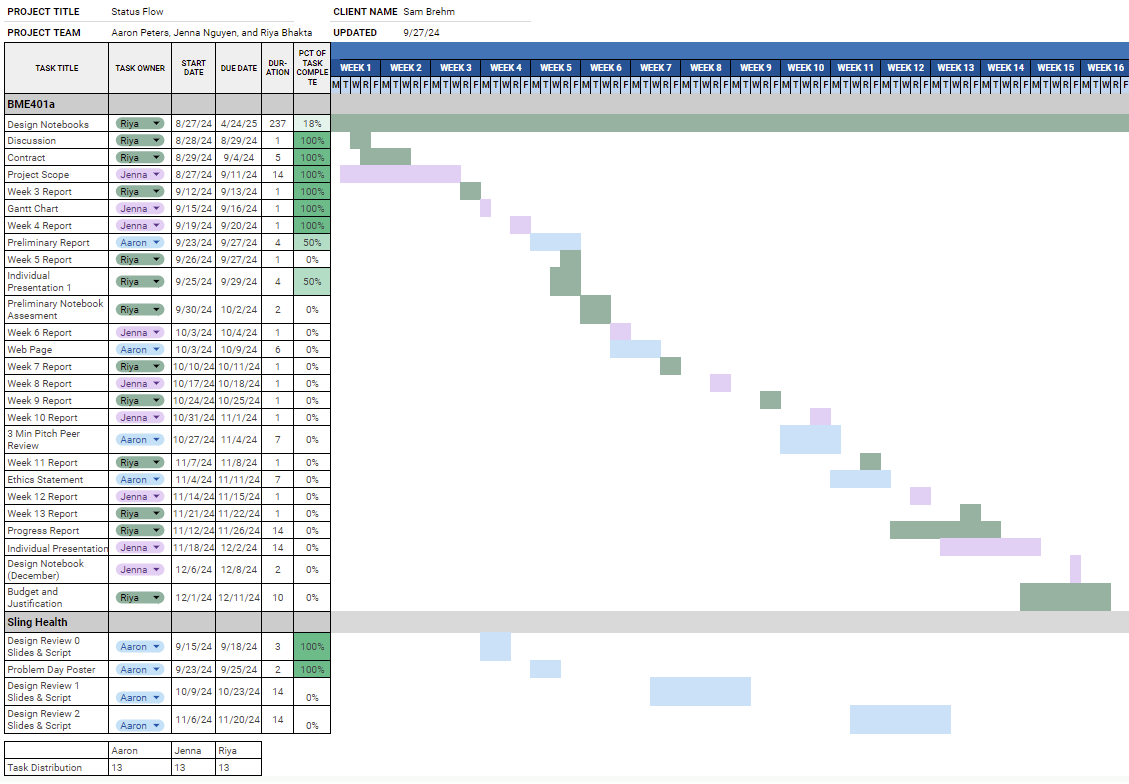
Figure 2: Fall 2024 GANTT Chart with Task Distribution Chart
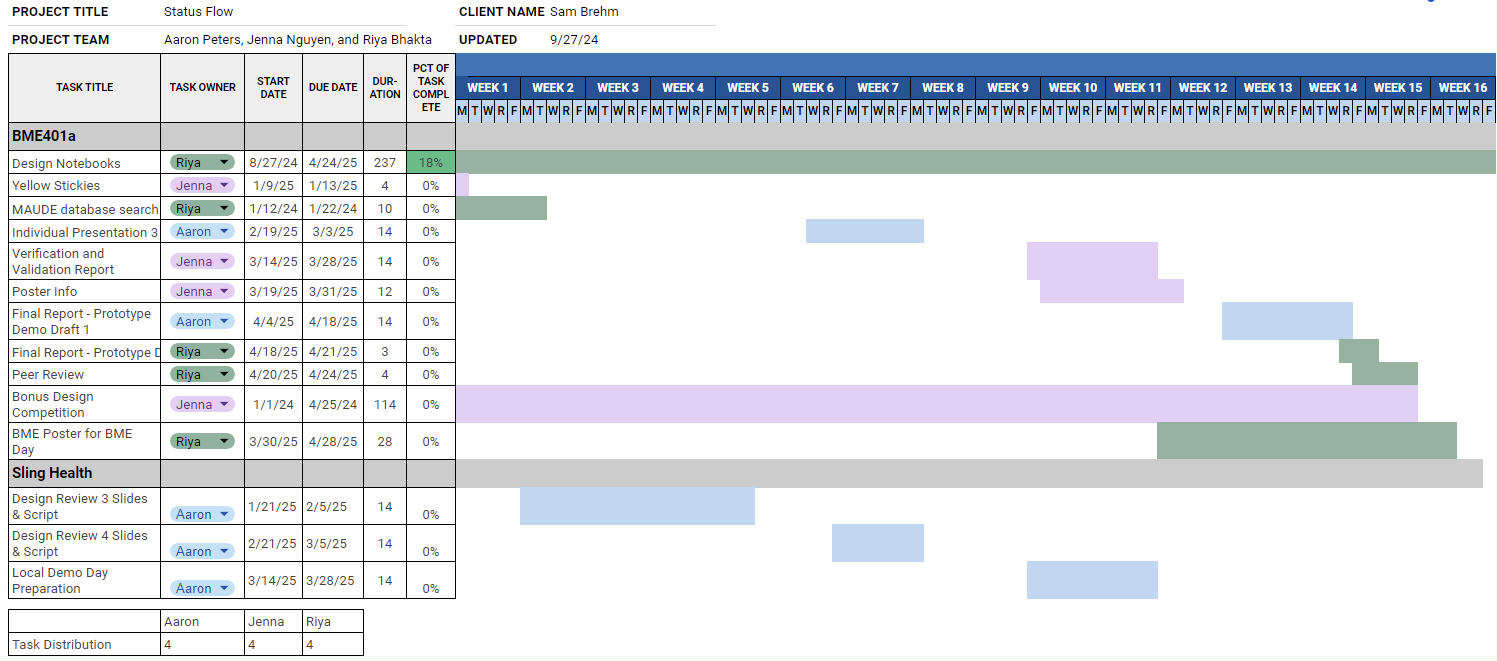
Figure 3: Spring 2025 GANTT Chart with Task Distribution Chart
Preliminary Simulation
To determine the feasibility of a spiral-shaped flow redirector as a solution to the problem described in the problem statement, preliminary simulations of the effect of spiral flow on wide-neck MCA bifurcation aneurysms were conducted using MATLAB and the parameters shown in Table 4 below. The simulation format is shown below in Figure 4. The results of the simulation are shown below in Tables 5 and 6.
Table 4: Parameters Used for Simulation
| Parameter | Value |
| Grid Size | 0.00028 |
| 𝜌 (density) | 1000 g/cm3 |
| 𝜇 (viscosity) | 0.003 Pa·s |
| Flow Type | Laminar |
| Inlet Velocity* | 0.583 m/s |
| Outflow Pressure | 0 Pa |
| Boundaries | Rest, no slip |
Table 5: Simulation Pressure in Pascals with and without the spiral flow redirector
| Pa | N | Min | Max | Mean | Std |
| No spiral | 621 | 693.482 | 795.231 | 728.231 | 19.1605 |
| Spiral | 608 | 348.23 | 369.96 | 366.084 | 3.9106 |
| Difference | 362.147 (p~0, 49.75%) |
Table 6: Simulation Volumetric Flow in m3s With and Without Spiral Flow Redirector
| Condition | Volumetric Flow (m3/s) |
| No spiral | 1.368*10^-6 |
| Spiral | 6.574*10^-7 |
| Difference | 7.106*10^-7 (51.93%) |
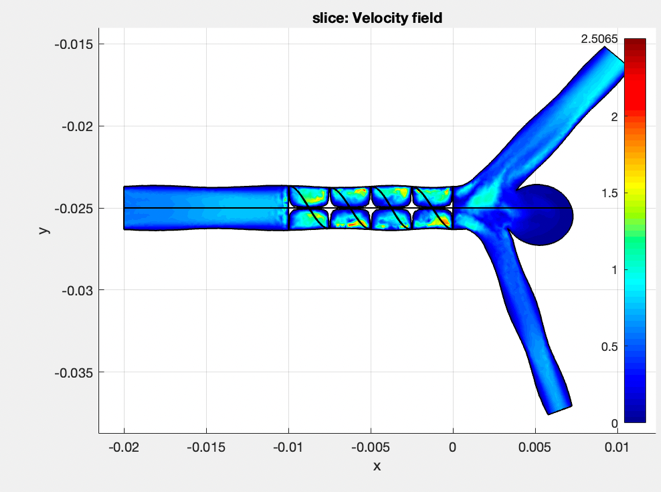
Figure 4: MATLAB Spiral Flow Simulation Format
References
[1] Wang, S., Li, L., Gao, H., Zhang, K., Shao, Q.-J., Li, T., & Gao, B. (2023). Middle cerebral artery bifurcation aneurysms are associated with patient age, sex, bifurcation angle, and vascular diameters. Scientific Reports, 13(1). https://doi.org/10.1038/s41598-023-50380-1
[2] U.S. Department of Health and Human Services. (n.d.-a). Cerebral aneurysms. National Institute of Neurological Disorders and Stroke. https://www.ninds.nih.gov/health-information/disorders/cerebral-aneurysms
[3] Maud, A., Lakshminarayan, K., Suri, M. F., Vazquez, G., Lanzino, G., & Qureshi, A. I. (2009). Cost-effectiveness analysis of endovascular versus neurosurgical treatment for ruptured intracranial aneurysms in the United States. Journal of Neurosurgery, 110(5), 880–886. https://doi.org/10.3171/2008.8.jns0858
[4] Iwakami, T., Fujii, N., & Son, J. (2021). Comparison of the physical characteristics of support stents for cerebral aneurysm embolization. Journal of Neuroendovascular Therapy, 15(12), 778–786. https://doi.org/10.5797/jnet.oa.2020-0167
[5] Gunnal, S., Farooqui, M., & Wabale, R. (2019a). Study of middle cerebral artery in human Cadaveric Brain. Annals of Indian Academy of Neurology, 22(2), 187. https://doi.org/10.4103/0972-2327.144289
[6] TonnTM Novatech® stent applicator. Novatech SA. (n.d.). https://novatech.fr/en/instruments/-bronchoscopy/tonntm-novatechr-stent-applicator
[7] Reynolds, M. R., Pinto, D. S., Shi, C., Walczak, J., Berezin, R., Holmes, D. R., & Cohen, D. J. (2007). Cost-effectiveness of sirolimus-eluting stents compared with vascular brachytherapy for the treatment of in-stent restenosis. American Heart Journal, 154(6), 1221–1227. https://doi.org/10.1016/j.ahj.2007.07.033
[8] Zhou, Z., Lan, W., & Yu, J. (2023). Endovascular treatment of middle cerebral artery aneurysms: Current status and future prospects. Frontiers in Neurology, 14. https://doi.org/10.3389/fneur.2023.1239199
[9] Kashkoush, A., El-Abtah, M. E., Petitt, J. C., Glauser, G., Winkelman, R., Achey, R. L., Davison, M., Abdulrazzak, M. A., Hussain, S. M., Toth, G., Bain, M., & Moore, N. (2023). Flow diversion for the treatment of intracranial bifurcation aneurysms: A systematic review and meta-analysis. Journal of NeuroInterventional Surgery, 16(9), 921–927. https://doi.org/10.1136/jnis-2023-020582
[10] Statistics and facts. Brain Aneurysm Foundation. (2024, August 27). https://www.bafound.org/statistics-and-facts/
[11] Billinger, S. A., Craig, J. C., Kwapiszeski, S. J., Sisante, J.-F. V., Vidoni, E. D., Maletsky, R., & Poole, D. C. (2017). Dynamics of middle cerebral artery blood flow velocity during moderate-intensity exercise. Journal of Applied Physiology, 122(5), 1125–1133. https://doi.org/10.1152/japplphysiol.00995.2016